There are areas where everything is getting worse, but now much progress is being made - speech / text recognition, translations.
But there are mysterious areas. It seems like there is progress. And articles are regularly published. Only now it doesn’t really get to practical use.
Let's look at how neural networks and machine vision work in medicine.
A small reservation . In the article I will only talk about machine vision. This is when we try to recognize something by an X-ray, a photograph, a picture with an ultrasound scan, CT / MRI, etc.
These are areas that have greatly improved in recent years. In other areas, everything is somewhat more confusing / cunning, I do not want to touch them.
Small disclaimer 2 . I want to do without explicit examples here, considering the communities that are true for almost all neurons. If you are interested in reading what neurons have recently learned to do in medicine, then I advise you:
Fluorogram recognition
Mammogram Recognition
Retina
Skin cancer
And much more.
Part 1 - with a swoop
Medicine is a very specific area of human knowledge. Unlike what I listed above (biometrics / numbers / translations) - there is a responsibility. If the doctor clearly messed up - human society suggests that he should fly. Not to say that this installation is always performed. But there is a certain paradigm in the minds of doctors and in the minds of society. Whoever you talk to, people always think in that framework.
And now we come with our neural net. And we say: “we predict with the same accuracy as the doctor!” (Below we will consider this statement in detail). The doctor looks at one photo - approx. The second is gorgeous. But on the tenth, he does not agree with the opinion of the network radically. The doctor would write “suspiciously,” and the network says “healthy.” “What is this ?!” the doctor thinks. “Would we really let this patient out ?!”
Globally, with the “neural network + doctor” approach, where the goal of the network is “to search for pathology,” the posterior distribution can be as follows:
- The patient has a pathology -> the neural network found her -> the doctor saw her (plus the doctor’s karma)
- The patient has a pathology -> the neural network did not find it -> the doctor saw her (the doctor believes "well, they came up with crap here", minus the network karma)
- The patient has a pathology -> the neural network could not find it -> the doctor also does not see anything (everyone was hollowed out, no punishment to anyone)
- The patient has a pathology-> the neural network did not find it -> the doctor doesn’t see her (the doctor thinks “well, they came up with crap here”, and then the two options are “the doctor is sure that he’s right”, the find goes to junk and “the doctor wants to push off the responsibility” - the appointment of additional analyzes / additional studies - and then victory)
- The patient has no pathology -> the neural network could not find it -> the doctor also does not see anything (plus the doctor’s karma)
- The patient does not have a pathology -> the neural network did not find it -> the doctor sees something ("what is your neuron does not see such obvious symptoms, even if there was no pathology here - definitely need to be checked!")
- The patient does not have a pathology -> the neural network found it -> the doctor also found something (everyone agrees, everything is in plus)
- The patient has no pathology -> the neural network found it -> the doctor does not see anything (again, there are two versions of the events “the doctor believes that he is right” - and everything is ok “the doctor wants to push off the responsibility” - and starts a chain of studies. The result is an annoyed doctor, that again I had to appoint a bunch of tests and there’s nothing).
Let’s now summarize all the outcomes: 1,3,5,7 - there is no change in the current study protocol. For screening studies, this will be 95% of cases. The neural network does not change anything, and any actions associated with it will complicate the work of the doctor => in the global sense they will put pressure in the negative.
Points 2 and 6 give an awesome minus to the karma of neural networks. They will create a clear negative every time they occur.
Point 4 is the only situation when a neuron can recoup. But she must go through the doctor’s negativity. And it will be completely killed by Paragraph 8 . In order for doctors to understand that the neuron is effective, the number of cases described in paragraph 4 should be comparable or higher than in paragraph 8. But this is achievable only in cases where the number of patients with pathology is high. For screening, this does not occur.
Reality looks even worse, to be honest. If the neuron sees what was not in the training, but which is unambiguous for the doctor, she will give out some random answers. Well, for example, the remains of complex medical interventions during fluorography (sutures / dentures / fragments). And, even if the network is statistically better than the doctor, but every couple of weeks the doctor sees the same obvious error - he will burn.
OK. We came to the conclusion that when integrated with a qualified doctor, the neural network is practically not able to increase the detection of diseases - it will only add problems. And let's think about how a neuron can be screwed up without a doctor? The real problem of clinics in Russia is a lot of low-quality local specialists. I spoke with doctors of the federal cents - and there are two complaints:
- Doctors at the slightest doubt send to the federal center for diagnosis
- Doctors do not see tumors on the chest floor (little experience)
It must be understood that in such situations, any neural network produces accuracy an order of magnitude higher than such a doctor.
But when you try to attract to reality, everything becomes a little sadder:
- Legislation will not allow to replace a doctor entirely - again, “who will be responsible”
- A low-level doctor will likely follow one of two paths:
- Consider yourself smarter than the network and not listen to its decisions. Judging by what I saw - there will be the majority.
- Fully comply with her decisions. This is not bad, but we cannot force the doctor to do it bureaucratically, because the doctor is the one who is responsible.
- At a low level, there are quite good doctors - and this must be taken into account. Such doctors can undermine the reputation of any program, indicating its errors.
The saddest thing is that this problem of “low qualification of a doctor” is solved in other ways, not in neural networks. A competent systematic approach, with constant training of a doctor / proficiency testing / creation of a network infrastructure so that one doctor can serve many hospitals at once / duplication for 2-3 doctors. Solving this problem with neural networks is about the same as approaching car repair with the words "I have a roll of scotch tape, why not try it."
The same DIT in Moscow is also on the path "first we will reduce everything to one place, and then recognize it." They promoted their decision with neurons at conferences. But they begin to work precisely with system solutions. Neurons will come to such places later, somewhere speeding up work, somewhere improving quality. It is necessary to start with the infrastructure.
Of course, there is a way how you can plug this problem in part with a neuron. Automatically check all the pictures taken in the institution. Set a threshold in such a way that there are almost no false positives (yes, let 20% of patients be skipped). And, if we are sure that the patient is sick, then, bypassing the doctor, assign him additional examinations.
It looks simple. In reality, this is a hellish option: it destroys the logic of decision-making (the patient was released, how to call him now), he destroys the reputation of doctors (how does Vasily Petrovich mow it ?!), he is unacceptable to the administration (how to skip 20% ?!). He will not work if the doctors are competent. The hospital does not understand the profit of this system, why spend money on installation. And it is possible only if the medical institution already has a good information system.
But, half of the projects I came across look in this direction ...
Another good option is to highlight the doctor what the network sees. Tumors / organs / some characteristics. But this is not a priority. And first of all, equipment manufacturers need it. At some point, such “assistants” will be able to pass the standard in the field. This approach does not require strict licensing, partially relieves the doctor, is a good competitive advantage for the device / software. I have seen several such projects. But, again, this is about something else. This does not replace the doctor, does not improve detection.
Part 2. And what about the statistics
Recently, an awesome article came out. A meta-study on what accuracy neural networks achieve and how it fights people. It does not contain answers to how something can be implemented / used. But at least it allows you to evaluate the modern cutting edge in science.
The final schedule of the article is approximately as follows (accuracy rating for all studies):
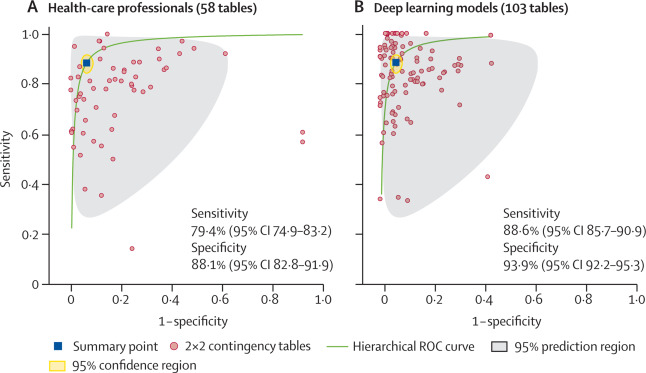
It seems that even people significantly lose! But do not forget that this is a meta-study, where the points on the graph are the final accuracy of the algorithms.
If we leave those articles where the assessment of people and the algorithm is based on an identical data set (there are only 14 of them), then the final graph will be much more interesting:

It can be seen that with an adequate comparison, the algorithms yield almost the same accuracy that professional doctors give.
But do not forget a few points:
- You can only train a neuron in a clearly defined task. If suddenly there is some strange crap in the picture, the doctor will immediately understand, and the output of the neuron will not be determined
- The accuracy of the doctor depends on the qualifications. This will be an example below. The neuron is likely to give some average accuracy.
- The neuron may be dependent on the method / on the training set. Doctor invariance is much greater.
About the accuracy of doctors. I came across several studies where they analyzed the accuracy of doctors. In fact, a really good neuron cannot be made without such a study. Of the latter, I really liked this one . Reading mammograms is one of the most difficult areas in radiology. It is necessary to spatially restore 4 images taken from different directions and understand whether everything is OK or not. A neuron gives somewhere 87% accuracy in the classification of sick / healthy. Doctors - from 70% to 86%. Moreover, according to the study, doctors had experience in this task.
No need to generalize this study to all other tasks. But a cool moment is visible - "the neuron definitely helps bad doctors." But the good ones are a little slow.
Part 3. About where neurons in medicine really help
All that I said above was a discussion on the topic of "neurons and the search for pathologies." Let's digress for a few minutes and talk about a more general topic - neurons and medicine. Can neurons help in medicine, in image analysis?
And here the answer is definitely yes. And it is already actively used. From the latest examples that came across (I bring here Russian purely medical startups that have reached the product):
UNIM is a network of laboratories performing research on biopsy specimens (doctors call this pathological research). These studies are quite long and dreary. The doctor sits down and counts the number of cells of one type, another type, the number of stained cells, etc. Just a couple of years ago, all these calculations were done under microscopes and with a counter in hand.
This is solved quickly and well through neurons. The accuracy is increased (something is already possible and the number of cells is algorithmically counting much easier than with the eyes + you can process a larger area in less time). And most importantly - the doctor’s work time is greatly accelerated.
DiagnoCat - CT scan for dental disease. A person has a lot of teeth. The attending physician usually pays attention to the tooth that heals + for what catches the eye. No one describes all 32 teeth fully. But the algorithm can. This approach increases conversion, improves the final condition of patients.
Only in Russia did I see 3-4 more companies / startups that successfully introduced machine learning into near-medical technologies. And these solutions have improved the quality of services / reduced their price.
The main feature of such startups is that they do not come from “solving all problems”, but from “speeding up data processing” / “improving efficiency”.
Epilogue
Neural networks now do not come from an idea like “but let's recognize X”. And from an idea like “we spend a bunch on Y -> can we somehow optimize this?”. Well, for example, automatically fill out a diagnosis if we spend a lot of time on scribble. Unfortunately, many do not understand this.
Will medicine change in the next 10 years? I think yes. But not due to neural networks, but due to informatization. Automatic flow control, virtual workstations, combining all data into a common database. And machine vision ... It will itself appear in those projects that will grow before it. Quiet and quiet.