Innervation of the eye: how the vision control network is arranged
Today I will talk about why, when you tilt your head, the eye automatically turns to a given angle with very accurate synchronization without losing objects in focus. Even as we, doctors, we connect the current to the nerves and “ring out” the circuit in order to understand that everything works. And about what will happen if sections of this chain are cut off or damaged.
Forgive me, fellow scientists, for simplifications and non-canonical terminology.
Well, I also answer the question when to remove a healthy right eye, if a patient has a serious infection on the left.
Data and management
Two networks are connected to the eye: motor and sensitive. Feel how unscientific it sounds, right? Because all this is called quite differently, but, in fact, this is exactly what works. As I have already said, I immediately apologize - I am more interested in practice, because I am a doctor, not a researcher.
The sensitive network transmits data (including the video stream from the retina itself and sensations from touching the eye), and the motor network transmits control signals. These networks are connected and have intersections in the form of reflex arcs. Reflex arcs (again, simplifying) are the means for executing some simple programs without involving higher in the hierarchy of ganglia.
When you touch the hot, then first withdraw your hand, then think. This worked the reflex arc from the sensitive system of the hand (exceeding the temperature threshold) to the motor (if this “sensor” speaks of problems - immediately pull on yourself!). Bundles are made on the nuclei of the nerves - nodes of the network.
From the sensitive part of the trigeminal nerve impulses can be transmitted into the facial nerve and descend through the motor fibers to the muscles. Without the participation of the brain, of course.
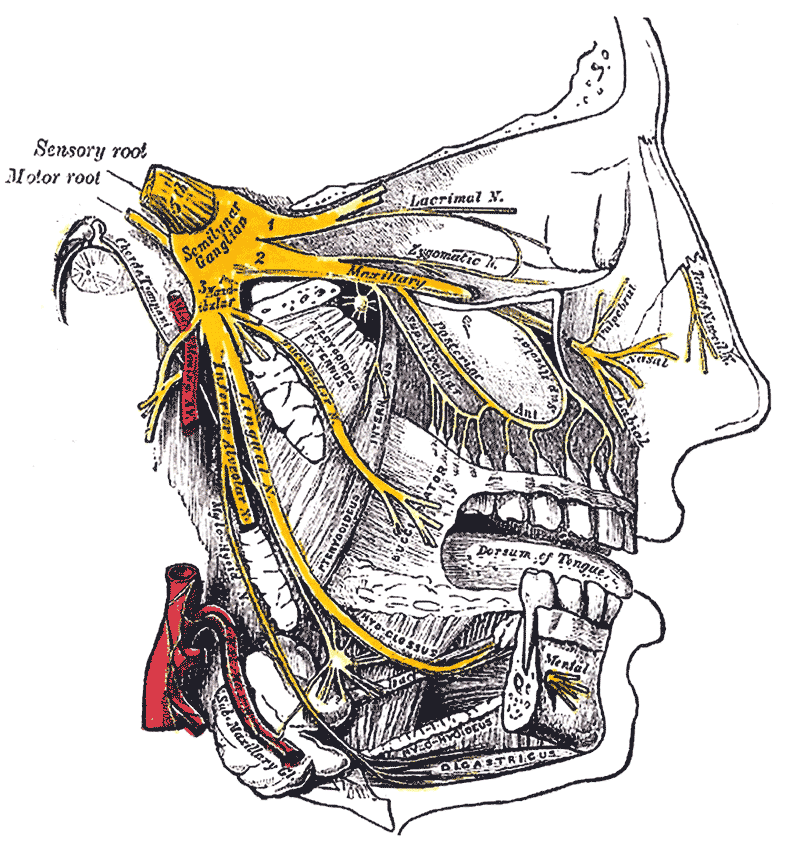
The trigeminal nerve innervates the entire face and part of the soft tissues of the cranial vault, it is he who is in the picture above the post. In the brainstem, it starts from two nuclei: sensory and motor. It has three main sensitive branches (and therefore trigeminal). The first branch is the back of the nose, forehead, upper eyelid and eyeball. The second is the maxillary sinuses, the teeth of the upper jaw. The third - the lower jaw, skin, gums.
In practice, it is important that the inflammation around or behind the eye, in the cavity of the orbit will be felt, the data collected and conveyed to the nodes in the upper part of the hierarchy - the nerves gather and go into the cavity of the skull and base. If the sensitivity breaks - it will noticeably over the centuries what is going on, they seem to be numb, as if not their own. If neuralgia starts, it hurts and hurts the whole face. If the herpes settled in the node of the trigeminal nerve, it can descend along the branches and pour out on the eyelids and nose wings. Even on the cornea that ends sadly.

Information flows
The reflex program can be, for example, such. If there is a grain of sand in the eye, the data on pain or discomfort through the branches of this trigeminal nerve enter the center of sensitivity (upper node of the network). There, data through the neural network is sent to the nucleus of the facial nerve in the brain stem. Creates a team that provides blinking and tearing. If something goes wrong, the information rises higher and higher, until you take a conscious effort to look in the mirror and pull the eyelash out of the eye with your hands. If the automation fails, we must think. The evolution to this was a long time.
The facial nerve is primarily responsible for movement (on the basis of the brain, an intermediate nerve is connected to it, which is responsible for gustatory and secretory functions). He is also amazing in many ways and very well thought out. For example, muscle contraction in one of its branches (to blink due to dryness in the eyes, this happens every 3-5 seconds) is arranged so that these same muscles squeeze the glands in the eyelids at the same time. The glands (meybomium and Zeiss) eject during this compression a secret, that is, a small amount of the lipid fraction of the tear film. On relaxation, a tear point is opened (the entrance to the tear bag), through which the tear goes into the nose (its lower course). It turns out that the muscle constantly pumps a tear and removes it, and the nerve controls this pump.
For the lacrimal gland there is a separate branch (the same intermediate nerve) that is part of a reflex arc with sensitive branches of the trigeminal nerve, coming from the nasal mucosa. So if you smell pepper, tears will go along with the snot. And life hacking is in that not only it hurts to beat in the nose, but also it is insulting - even healthy men cry. I do not know why you need it.
We now turn to the interesting. Look at the picture. So far nothing is understood on it, but it will come in handy further:
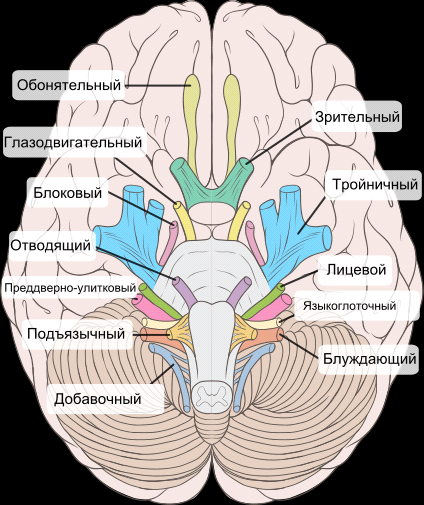
Motor innervation is not only open-close eyes. This is another movement to the side, turning the eyes up and down. There is a separate block nerve, it goes into the cavity of the orbit of the eye and innervates the superior oblique muscle, it lowers and leads the eye out. And the abducent nerve pulls the eye out: it is an independent nerve and a separate muscle. The remaining 4 muscles control the turns of the eye are controlled by the oculomotor nerve.
If we were to design a person from scratch, you probably would have to do one system. But since reptiles, something has already gone wrong, so there are separate nerves connected by a very extensive network of reflex arcs. All eye positions are regulated consciously and unconsciously, and when you turn the eye, three different ways are used unconsciously to control the muscles.
Complicated management
The control centers of the movements are levels higher. In the frontal lobe of the brain (the base of the second frontal gyrus) is the center of conscious eye coordination, when you clearly want to turn the eye on the results of long-term reflections.
The second center in the occipital lobe - involuntary eye movements. When you tilt your head, the eye turns immediately to the desired angle. For this, the nerve core “removes” the data from the vestibular apparatus and, through the reflex arc, transmits the control signal to the rotation of several muscles of both eyes at once.
In children, we check the involuntary movements of toys. We show a bright interesting toy, then we hide and lead from the blind zone into the field of view. If the child turns her head, everything is in order, the occipital centers have worked.
The frontal center has a higher priority compared with the occipital. If we look closely enough at a specific object, and a car is driving alongside, then the frontal center prohibits being distracted by such a big, fast and beautiful, although it is a reflex. Therefore, the most attentive gophers get a bumper on the head.
There are also cortical centers responsible for complex states of reading, pattern recognition, assessment of what they see, and visual memory. The connection between the cortex and the nuclei of the corresponding nerves passes through the thalamus. This is a cluster of gray matter, a structure in which processing and integration of almost all signals takes place so that the process goes smoothly and continuously. Very difficult place to manage.
If a patient has a nail in the head and hit the frontal lobe (or inflammation has started, or insufficient trophicity, a tumor, complicated poisoning - in general, many causes of damage), he cannot consciously look at any object, uncontrolled stereotypical movements appear (and not only the eye, yes, there will still be many other violations). If the occipital - consciously can, just do not understand what he sees, or hallucinates.
Nervous network resistance to damage
Now, about how fast and accurate unconscious control. To look to the left, you need to use both nerves - the oculomotor and the abductor, because one eye must be brought to the nose, the second taken outside. Accordingly, these nerve fibers must be synchronized. When such a connection is broken (and both nerves are in order - not uncommon for hemorrhage, injuries, multiple sclerosis or stroke), then consciously creating a movement “to look at the car driving on the left with both eyes” will not work out, only one will move, and the second stand still, an annoying double vision will appear. Then the patient adapts, the neural network begins to redistribute functions, information in the brain is overestimated - and the signal from the left or right eye, and not a combination of pictures, can be given more importance.
The position of the eye makes it easy to determine which of the nerves has suffered, for example, after an accident or a stroke. If the eye is looking directly into the nose, this is damage to the abducent nerve. If the nose on the characteristic diagonal - damage to the block. Damage to the oculomotor - this eye looks out, down, covered with a century more than healthy, and hurts. Facial - the eye dries and is bad or does not close at all.
In a patient coma, almost nothing works because of the inhibition of the function of the cortex, subcortical and stem structures. It may be sudden or develop gradually. The preservation of reflexes can be estimated coma depth. There will be residual reactions, for example, if you pull the tweezers behind the eye, there will be a slight trembling of the eyelid, and the pupils continue to taper to light.
In patients with consciousness, signal disturbance also sometimes occurs. In this case, we ourselves can do little - not quite our profile. We are responsible, in fact, for the video camera, not the wiring and hub. Therefore, we go to our analog electrician-setevika - to the neurologist. He has a special device for electroneuromyography - he helps to explore the electrical potentials of nerves and muscles with the help of various influences (often a weak electrical discharge). All this is accurately measured. If the impulse passes, then the nerve is almost in order. We usually bring the result, and we continue to work, thinking that such a result could cause and how to treat it.
But there are cases when it is impossible to measure this way. We did not climb into the eye with such a device, so another method is applied. For example, in case of loss of the visual signal, it is necessary to find out what it actually was: nerve damage or processes on the retina, or in general behind the eye. Using electroretinography or visual evoked potentials, one can estimate the level of the lesion, whether it is necessary to perform an operation (or it makes no sense if there are problems on the nervous network).
The fibers from the retina unite in the optic nerve and go through the head to the back of the head into the visual cortex. Over the pituitary (in chiasm) part of the fibers intersect and change sides - it is necessary to synchronize the left eye and right, in the “right” picture there is a piece of information left, and in the “left” - part of the information right, so the brain knows exactly where and what It depicts how close it is and also allows you to estimate volume. Then the fibers go to the lateral articulate body, receive the primary signal processing at the thalamus and the upper quadrilateral nucleus, then the fibers are fanned into visual radiance, going through the temporal lobe to the visual cortex.
Accordingly, the trauma of the temple - the patient does not have a piece of visual field. Each place of defeat has its own characteristics. If before the intersection - the field fell out only from one side affected. If the problem is in the crossroads area, then external or internal pieces fall out from two sides. More often outside. If at the level of the visual cortex - most often the “dropped out” point with one and symmetrical with the other. There are partial damages - there will be segments that are symmetrical to the left of the nose, to the right of the temple, but shifted in one direction. When a stroke in the corkscrew area often falls to the left a small piece. Evaluation of visual fields gives a lot of information both to us and to neurologists.
And finally - about one of the most irrational behaviors of the immune system. Situation: the eye is damaged before the rupture of the membranes (for example, a piece of glass has entered). The immune system does not even know that there is an eye in the body, it is arranged this way. But when the sclera is torn, the pigment epithelium of the retina and other proteins begin to enter the blood. From the point of view of the immune system, all these details are not from our body. Immunity begins to remove them. But he is smart, and sometimes even too — quite quickly the whole organ is found, which consists of the same proteins, which means it “harms” the body. This is the eye. And begins a crusade against him. But again, the immune system is smart. She also finds the second such organ - and in any case attacks her. And changes in a healthy eye can begin in 3 and more weeks after damage of the first. Therefore, with injuries, severe uveitis and endophthalmitis, we observe the patient regularly, look at the antibodies, so as not to miss the moment.
Something like that. Now, according to the anecdote, “your eyes are like conscripts: one is mowing, and the second is blue,” you can roughly make a diagnosis. Just do not treat, carry the patient to the hospital.
Be healthy!
All Articles