Laser vision correction SMILE or "Why we do SMILE"
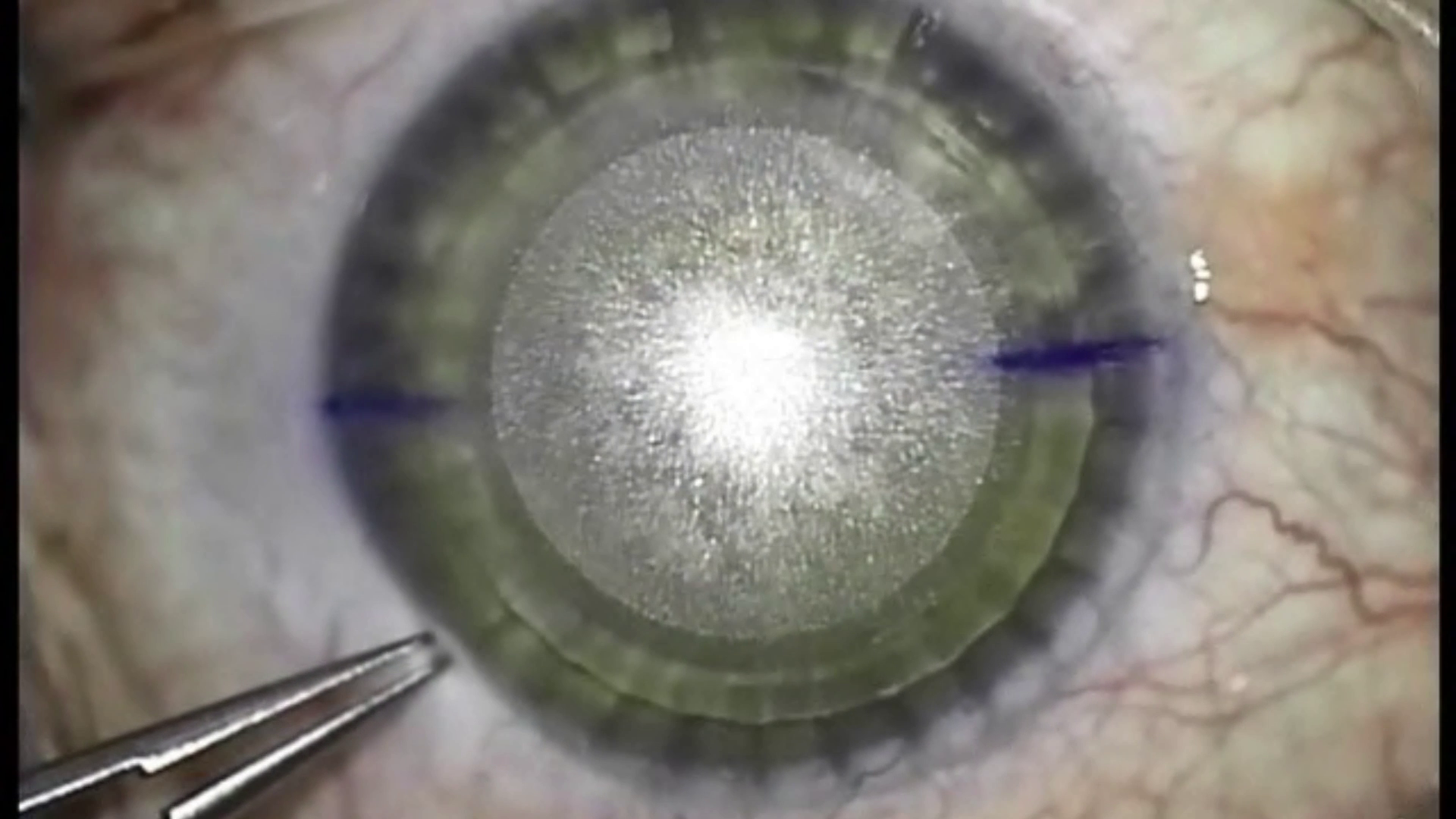
Cornea after laser incision
To date, discussions on the topic “Which method of laser correction is the best?” Are increasingly arising in the Internet space. For a long time, I didn’t want to intervene in an insignificant discussion, but, seeing the regular comments of the “crusaders against SMILE” from the clinic, who do not have the technical ability to do operations like SMILE, still could not stand it. Communicating with colleagues from Germany during one of the scientific conferences I heard an interesting phrase: “the introduction of something new meets competition in three phases of development:
- Not given any attention, because "all the same is nonsense"
- Actively attacking or denying a competitive product is what we encounter in online posts.
- Complete calm, during which the development of their own products of this type is being conducted - this is how Alcon and Schwindt companies, which now develop the SMILE technology, reacted in due time.
Apparently, such errors are encountered not only in commercial companies, but also in individual Russian surgeons.
To begin with, the operation Femto-LASIK is a really good and justifiable method for years, which I have mastered for many years. Therefore, the question is not in the confrontation of these operations, but in the choice of the best technique for an individual patient depending on his age, refraction and other factors.
Being an active user of SMILE technology, I want to respond to the comments of colleagues of ophthalmologists, based on data in the reviewed world scientific literature, possibly meta-analyzes, in which all the studies on this topic are compared.
Here are the arguments that are unreliable in terms of evidence-based medicine:
Myth 1. The risk of dry eye syndrome after SMILE surgery is no less than after Femto-LASIK, since the SMILE process produces a rather long vacuum on the conjunctival goblet cells responsible for the production of tears and corneal nerve fibers are damaged. .
Answer: Unfortunately, you are wrong. The conjunctival goblet cells are destroyed by femtosecond lasers with a conjunctival capture zone (for example, the devices of the companies Intralase (AMO), Wafelight (Alcon), etc.). VisuMax has a purely corneal grip (see Figure 1) and therefore cannot influence the cells of the conjunctiva! Reducing problems with dry eye syndrome is associated with a small lateral incision. By the way, I work with a 2.5mm rather than a 3 mm slit - compared to a 20 mm slit with Femto-LASIK. On this subject there are scientific papers. A meta-analysis on this topic confirms the theory of denervation: in the initial period, problems with SMILE are less. After 6 months there is no difference between the two operations, since Femto-LASIK is regenerated during this time.
Myth 2. Correction accuracy at SMILE operation is significantly lower than with Femto-LASIK; it does not correct hyperopia, mixed astigmatism and high degrees of myopic astigmatism. The SMILE operation does not allow for personalized ablation, taking into account the individual characteristics of the cornea.
Answer: The accuracy of the correction after SMILE is not a bit worse than the aspherical profiles of an excimer laser. And on this topic there are already many publications that are in the meta-analysis. Despite the fact that some studies show some advantages of SMILE, and some of Femto-LASIK, there is no difference in the total comparison. I think that colleagues in this statement relied on some of the reviews of doctors, recently engaged in technology SMILE. They do not have their own SMILE nomograms, while Femto-LASIK has been involved for a long time. In addition, surgical skills with SMILE are much more important than with Femto-LASIK. By the way, this was also one of the factors why we decided to join the network of SMILEEYES clinics. Doctors in SMILEEYES have many thousands of experience and a huge database that we use. Moreover, the training was conducted by the pioneer of technology, Professor Walter Sekundo, who himself operates several times a year in Moscow. Thus, we did not even have a single case of the need for additional correction. According to the literature, the need for additional correction after SMILE is 2.2%, and after LASIK from 5 to 8% and this is not connected with Femto-LASIK’s inaccuracy (it is quite accurate), but with regression, which is more with Femto-LASIK than with SMILE.
Colleagues are right that at the moment the correction of hyperopia and mixed astigmatism for commercial purposes is not possible. In May this year, prof. Sekundo and co-authors, as well as Reinstein and co-authors, 8 presented the unusually successful results of the study of hypermetropia and astigmatism correction at the Los Angeles conference (ASCRS = American Society of Cataract and Refractive Surgeons). Admission for commercial use is expected 3 years after the end of a multi-centered international study led by Secundo. As for myopic astigmatism - should argue with colleagues. As surgeons who have no experience with SMILE, they are apparently not familiar with the latest publications on corneal marking for high astigmatism (Ganesh S, Brar S, presentation on APACRS 2017, also Fig. 1). The clinics of the SMILEEYES group immediately adopted this innovation and the results are really extremely good.
Myth 3. During the SMILE operation, the optical zone decentration may occur significantly more often than during the Femto-LASIK operation, and sometimes, especially often when correcting myopia of a low degree, it is difficult to remove lenticules (lenses from the optical zone of the cornea), which also negatively affects on visual acuity after surgery.
Answer: The tale that with SMILE more decentration or worse, centering is simply nonsense. Read the literature! Already in 2014, Lazaridis and Sekundo, and then in 2015, Reinstein and co-authors showed that skillfully performed autocentration (the patient looks at the flashing lamp and at the same time captures the cornea) is not inferior to excimers with an active tracker like MEL 80 and even MEL 90.
We in the Moscow branch of SMILEEYES (as well as our colleagues in European centers) perform correction of -1.0 diopters (we had patients with -0.75) - the laser allows you to do this myopia - with a phenomenal result. It all depends on the surgeon’s ability to use his hands, head and laser settings.
Myth 4. After the SMILE operation, wrinkling and opacities are possible in the central optical zone of the cornea, which permanently reduce the acuity and quality of vision (up to six months or more).
Answer: Colleagues are right. Of course, after myopic SMILE, microslips may appear because the surface of the “cover” after removing the lenticular more than the surface of the reduced corneal stroma. But after all, with LASIK, not only micro-tabs, but even macro-tabs can appear! (and they do not improve over time, so the patient should be put on the table again). Therefore, the last step in both operations is smoothing the surface.
Myth 5. Certain difficulties arise when it is necessary to supplement the refractive effect after the SMILE operation. In such cases, you have to switch to Femto-LASIK or PRK technology.
Answer: At this point, colleagues contradict themselves. Praising Femto-LASIK, they write, “Certain difficulties arise when the refractive effect is needed after refraction after refining. In such cases, you have to switch to Femto-LASIK or PRK technology. ” That is how: Femto-LASIK is great, but if SMILE should be transferred to Femto-LASIK, is it bad?
By the way, there is the possibility of an additional correction using the SMILE method - this is a regular CIRCLE module, but this is only suitable for large additional corrections, and there are such around the world, despite almost 800,000 (!) SMILE operations performed on the fingers.
Myth 6. And all the shortcomings of the Femto LASIK operation, such as the effect on twilight vision and the reduction of the corneal framework properties, are inherent in the SMILE operation almost to the same extent.
Answer: As for the limitations in the postoperative period, I fully agree with the opinion of my colleagues. I don’t see a big difference between the two types of operation - after SMILE one day is enough, and after Femto-LASIK two weeks are enough. However, for active people, a difference of two weeks may be significant! But the fact that the decrease in frame stability after SMILE is less, especially for large corrections, is indisputable and the colleagues here are completely wrong.
Let me finish this post with a request: let's move on to the third stage of the discussions (see above). SMILE is an advanced technology that has enriched the repertoire of laser-refractive surgical interventions, making them even safer and more comfortable. The question should not be that it is good, but it is bad, but that an individual approach is needed. And each method has its pros and cons. Therefore, Femto LASIK, SMILE and even PRK (especially for refractions in the region of 1 diopter) are able to exist next to each other.
Figure 1 shows the eye immediately after the laser cut. The prints of the suction cone are clearly visible on the periphery of the cornea. Pay attention to the marking of the axis, which allows for a precise adjustment of the high degree of astigmatism. (the illustration was given permission by Prof. V. Sekundo)
Literature
1. Shen Z, Zhu Y, Song X, Yan J, Yao K. Dry Eye after Small Inclusion Lenticule Extraction (SMILE) versus Femtosecond Laser-Assisted Eyelid Surgery (FS-LASIK) for Myopia: A Meta-Analysis. PLoS One. 2016 Dec 16; 11 (12): e0168081.
2. Denoyer A, Landman E, Trinh L, Faure JF, Auclin F, Baudouin C Dry eye treatment: comparative outcomesof small incision lenticule extraction versus LASIK. Ophthalmology. 2015 Apr; 122 (4): 669-76.
3. Shen Z, Shi K, Yu-Y, Yu-X, Lin-Y, Yao K. Small Incision Lenticule Extraction (SMILE) versus Femtosecond Laser-Assisted Shaping (FS-LASIK) for Myopia: A Systematic Review and Meta-Analysis . PLoS One. 2016 Jul 1; 11 (7): e0158176.
4. Liu M1, Chen Y, Wang D, Zhou Y, Zhang X, He J, Zhang T, Sun Y, Liu Q. Clinical Outcomes After SMILE and Femtosecond Laser-Assisted LASIK: A Prospective Random Comparative Study . Cornea. 2016 Feb; 35 (2): 210-6
5. Kanellopoulos AJ Topography-Guided LASIK Versus Small Incision Lenticule Extraction (SMILE) for Myopia and Myopic Astigmatism: A Randomized, Prospective, Contralateral Eye Study. J Refract Surg. 2017 May 1; 33 (5): 306-312.
6. Lazaridis A, Droutsas K, Sekundo W. SMILE for myopia and comparison with FS-LASIK: subjective versus objective alignment.J Refract Surg. 2014 Oct; 30 (10): 680-6
7. Reinstein DZ, Gobbe M, Gobbe L, TJ Archer, Carp GI.Optical Zone Center Accuracy Using Corneal Fixation-of-Eye SMTFL-Laser-assisted LASIK for Myopia. J Refract Surg. 2015 Sep; 31 (9): 586-92
8. Reinstein DZ, Gobbe M, Gobbe L, Archer TJ, Carp GI. Optical Scanning Laser Correction Laser-assisted LASIK for Myopia. J Refract Surg. 2015 Sep; 31 (9): 586-92
9. Donate D, Thaëron R. Preliminary Evidence of Successful Enhancement After the Primary SMILE Procedure With the Sub-Cap-Lenticule-Extraction Technique. J Refract Surg. 2015 Oct; 31 (10): 708-10
10. Spiru B, Kling S, Hafezi F, Sekundo W. Biomechanical Differences Between Femtosecond Lenticule Extraction (FLEx) and Small Incision Lenticule Extraction (SmILE) Tested by 2D-Extensometry in Ex Vivo Porcine Eyes. Invest Ophthalmol Vis Sci. 2017 May 1; 58 (5): 2591-2595
11. Kling S, Spiru B, Hafezi F, Sekundo W. Biomechanical Weakening of Different Slices. J Refract Surg. 2017 Mar 1; 33 (3): 193-198.
12. Osman IM, Helly HA, Abdalla M, Shousha MA, corneal biomechanical changes in the eyes of the keratomileusis. BMC Ophthalmol. 2016 Jul 26; 16: 123
2. Denoyer A, Landman E, Trinh L, Faure JF, Auclin F, Baudouin C Dry eye treatment: comparative outcomesof small incision lenticule extraction versus LASIK. Ophthalmology. 2015 Apr; 122 (4): 669-76.
3. Shen Z, Shi K, Yu-Y, Yu-X, Lin-Y, Yao K. Small Incision Lenticule Extraction (SMILE) versus Femtosecond Laser-Assisted Shaping (FS-LASIK) for Myopia: A Systematic Review and Meta-Analysis . PLoS One. 2016 Jul 1; 11 (7): e0158176.
4. Liu M1, Chen Y, Wang D, Zhou Y, Zhang X, He J, Zhang T, Sun Y, Liu Q. Clinical Outcomes After SMILE and Femtosecond Laser-Assisted LASIK: A Prospective Random Comparative Study . Cornea. 2016 Feb; 35 (2): 210-6
5. Kanellopoulos AJ Topography-Guided LASIK Versus Small Incision Lenticule Extraction (SMILE) for Myopia and Myopic Astigmatism: A Randomized, Prospective, Contralateral Eye Study. J Refract Surg. 2017 May 1; 33 (5): 306-312.
6. Lazaridis A, Droutsas K, Sekundo W. SMILE for myopia and comparison with FS-LASIK: subjective versus objective alignment.J Refract Surg. 2014 Oct; 30 (10): 680-6
7. Reinstein DZ, Gobbe M, Gobbe L, TJ Archer, Carp GI.Optical Zone Center Accuracy Using Corneal Fixation-of-Eye SMTFL-Laser-assisted LASIK for Myopia. J Refract Surg. 2015 Sep; 31 (9): 586-92
8. Reinstein DZ, Gobbe M, Gobbe L, Archer TJ, Carp GI. Optical Scanning Laser Correction Laser-assisted LASIK for Myopia. J Refract Surg. 2015 Sep; 31 (9): 586-92
9. Donate D, Thaëron R. Preliminary Evidence of Successful Enhancement After the Primary SMILE Procedure With the Sub-Cap-Lenticule-Extraction Technique. J Refract Surg. 2015 Oct; 31 (10): 708-10
10. Spiru B, Kling S, Hafezi F, Sekundo W. Biomechanical Differences Between Femtosecond Lenticule Extraction (FLEx) and Small Incision Lenticule Extraction (SmILE) Tested by 2D-Extensometry in Ex Vivo Porcine Eyes. Invest Ophthalmol Vis Sci. 2017 May 1; 58 (5): 2591-2595
11. Kling S, Spiru B, Hafezi F, Sekundo W. Biomechanical Weakening of Different Slices. J Refract Surg. 2017 Mar 1; 33 (3): 193-198.
12. Osman IM, Helly HA, Abdalla M, Shousha MA, corneal biomechanical changes in the eyes of the keratomileusis. BMC Ophthalmol. 2016 Jul 26; 16: 123
All Articles