How DOC + moves paper archives to tablets and smartphones
Remember the good old registry in the nearest clinic. It is terrible to imagine how much labor, effort and paper goes to maintain it. And this despite the fact that the paper archives continue to deteriorate and get lost.
Fortunately, they have a digital alternative - electronic medical records. In this article we will describe how they change the lives of patients and doctors for the better and how we use them to improve the DOC + service.
“ Remember your trips to the clinics. What annoys you about them? ”
Electronic medical records, or EHRs, are analogs of paper cards familiar to everyone, which are kept at medical facilities and issued at registries. In the world, they have been running for over 50 years. Their task is to simplify document circulation and reduce the volume of “paper bureaucracy”. The electronic database is easier for doctors to contact, it ensures the completeness of patient data and their safety (in comparison with a paper card that can be lost or messed up, accidentally drops the necessary certificate or a badly pasted sheet).
In the course of treatment or while the patient is using the services of the medical institution, all the same information is entered in the electronic card as in the paper archive - a history of diseases, a history of treatment, data on vaccinations made, and so on. All this information may be available to doctors, clients, and the clinic.
As an EHR product, it is not just a digital version of medical documents, but a full-fledged ecosystem. Doctors, patients and administrative staff work with her. All of them interact with one system, but with different levels of access depending on needs and / or official duties. An EHR for a doctor looks like an analogue of a paper call card with fields for collecting medical information. For the call recipient, as a log entry. For the patient - as his personal medical record.
For the patient, it is important that the EHRs guarantee the coordinated assistance of all specialists who have ever conducted its examination. Electronic cards provide access to a personal medical history with records in digital form for the entire period of treatment. EHRs reduce the likelihood of medical errors and improve the quality of medical care. The patient gets more control over the treatment process and over their own health - the collected data allow you to track the testimony for the last year or several years. This is useful in emergency cases, and in quite ordinary attempts to lead a healthy lifestyle.
An EHR physician is helped to make the most accurate picture of a patient in the shortest possible time - all data on past diagnoses and prescribed medications are collected in one place. While the doctor is on the way to a call or is waiting for admission in the clinic, he will already know whether the patient has chronic diseases or allergic reactions, which specialists he applied to and what was recommended to him.
For medical institutions EHR is a convenient way to work. Digital records allow you to store information with minimal risk of losing it, reduce the proportion of routine work, solve the problem of overcrowding of archives and help speed up and simplify interaction with other institutions, for example, with insurance companies and other clinics. Researchers at Baylor Scott & White Healthcare Medical Center concluded that the introduction of an EHR at their center helped increase the efficiency of the operating room and reduce the number of delays in preparing for operations.
The digitalization of healthcare (including through the introduction of an EHR) opens up the possibility of automatic data processing and collection of morbidity statistics, which, on the one hand, helps in planning, on the other hand, it increases the level of medical service. Electronic medical records make it easier to control the quality of services through standardization: digitized diagnoses and treatment plans are easier to check for compliance with medical care standards.
It is beneficial for both doctors, patients and clinics that EHRs guarantee the completeness of patient data and their safety. Studies show that large American clinics have reduced their costs by 3.4% three years after adopting the EHR. But in general, American hospitals expect to save up to $ 44 billion a year only due to the introduction of an EHR and a reduction in the number of routine procedures associated with sending, copying and storing paper documents about patients.
If you look wider, e-cards open up the possibility for data exchange between all providers in the health care system. There are already such projects - Taiwan has a system for sharing medical information, Singapore has a national program , and Estonia has a single electronic registry . This, quite likely, awaits us in the future.
Let's sum up the intermediate results. Here are the main advantages of EHR:
And also EHC is eco-friendly. According to the American company Kaiser Permanente, its electronic accounting system has helped to withdraw from circulation 1000 tons of paper documents and 68 tons of X-ray film. For comparison, it is as if 20 thousand Russians in a year would not have spent a single piece of paper.
Our doctors go to home customers, as well as conduct online consultations. For us, EHR is the basis of document flow and a guarantee of a quality service.
DOC + doctors do not take physical cards with them for calls, and the archive is 100% digital. However, by law, we are obliged to keep medical documents in paper form, so the minimum set of required documents is stored in our hub. But the most important thing happens on electronic platforms.
Since the launch of DOC +, the IT system has grown around the project. At first, it was supplemented by a website and applications for doctors and patients. At that time, we made the integration of CRM, call center and medical platform with the backend, and also introduced the prototype of EHR in the usual tables. However, we understood from the very beginning that we would need a complete solution for mobile and desktop devices.
We were guided by the following goals:
To make this possible, we needed the following basic functionality for doctors:
Patients should immediately have access to:
The first version of our EHR was focused on the work of pediatricians and therapists. In December 2016, ENTs and neurologists joined DOC +, it became possible to call a nurse and import laboratory test results. The architecture of the solution became more complex, and it became necessary to adapt the maps to the peculiarities of the new specializations. This led us to the creation of the EHC designer. Its development is the next stage of the project.
It took three months to create the first beta version of the EHR system. When she was ready, we moved on to designing a separate mobile application for doctors. Thanks to him, experts can fill the EHR on the service tablets with which they go on calls.
To ensure the safety of user data, all our tablets have a special certified software installed: Continent-AP, Kaspersky Anti-Virus, MDM-center. We made sure that a secure data channel remained between the tablet and our data center.
From the client application, the patient learns the diagnosis, the result of the examination by all relevant specialists and the history of calls. In the “Clinic” section, he becomes familiar with the list of our services, and “Chat” allows you to consult with your personal physician.
/ on the screenshot an example of the interface of a personal medical card (as an example, the data of a fictional user is shown)
The third type of EHR users, besides the doctor and the patient, is the DOC + call center operator. Card management begins with it. Each incoming application from the client - by phone, from the website or from the application - is automatically recorded in CRM. If the application is not received through a mobile application, the call center specialist indicates the name of the applicant and the patient, his address and the doctor’s specialization. If the client has already contacted us before, the name and address are filled in automatically. The operator remains only to clarify them.
As a result, several data blocks are formed at this stage: information about the application, composition of the application, payment information, information about the caller, information about the patient, address of the call with the card, information about the reason for the call, information regarding the disability sheet and the cost of transfer.
All entered data is automatically redirected to the system of auto-dispatching. It is called Mildly Intellectual Routing Algorithm or MIRA. MIRA assigns a specific doctor to the call. The doctor, in turn, receives a formed EHR and assigns the status “on the road” or “drive up”. The customer receives an SMS or push notification that the doctor will arrive soon.
After examining the patient and collecting anamnesis, the doctor fills out the first part of the data in the EHR: client's e-mail, information about referrals to tests or additional studies, diagnosis, and appointments. This information is sent to the client in the DOC + application. In CRM, the diagnosis and prescriptions are not drawn up - this is medical information that the call center operator does not need to know.
/ call window in the DOC + application for doctors (as an example, the data of a fictional user is shown)
In the client application destination appear instantly. The famous problem of "medical handwriting" disappears by itself.
After the call, the doctor fills the card in more detail. Forms of an objective assessment of the general condition of the patient during the inspection of 32 points, the state of the respiratory system on 22 points, the circulatory system on 20 points, as well as the nervous and urogenital systems, blocks of anthropometric data and recommended consultations of relevant specialists are formed. Now for the convenience of making these data provides a drop-down menu with options for answers.
The last stage of the life cycle of an EHR is checking customer well-being Now we are working on the “three calls” system: immediately after the call, in order to clarify how the reception went, in the middle of the recovery process and the final one - by the expected recovery time.
To find out about the client's well-being, call center employees call him on average three days after the inspection. During this time, you can evaluate the first results of treatment. We contact the patient in a convenient way. If he uses only the application, then we will not call him, but write in the chat.
If necessary, the client will be able to talk with the consulting doctor, and the doctor will see if the patient has passed the necessary tests, if he has undergone additional research at a partner clinic.
The part of the EHR that is filled in after the call is available to the doctor and the medical board.
The medical commission that controls the quality and safety of medical activities is made up of experts of the relevant specialty who check medical records: whether the medical history is fully collected, whether the prescribed treatment is appropriate for the diagnosis.
Cards are checked for verification by the medical board in an automatic mode, in an impersonal form and randomly. The completed EHR is sent to the common pool, from which the algorithm selects cards for experts.
The commission does not know the identity of the patient, whose card she checks, and the doctor who issued her. Only impersonal information is submitted to the court of experts: medical history, history of the disease, examination data, diagnosis, what treatment the doctor prescribed, what drugs were prescribed, what tests were suggested to be taken, what additional consultations or examinations to take. Verification is conducted by 20 criteria. Each of them is rated on a three-point scale: “fully meets the standards”, “partially meets”, “does not meet”.
The medical commission verifies the correctness of filling the EHR, the completeness of the examination and collection of anamnesis, the compliance of the diagnosis. At the end of the month, the doctor’s accumulative assessment of all his verified cards is considered. We get the assessment of each doctor, groups of doctors, specialties and, in general, all DOC + doctors in the context of different criteria. From the statistics, we learn how correctly doctors choose drugs and treatment. This assessment is used in the scheme of awarding doctors.
We have plans to make an EHR more convenient and useful for both the client and the doctor. Now we are focused on expanding the functionality of the cards.
A reference book of drugs has already been added, which contains INN preparations (international non-proprietary name), dosage and release form. After filling the appointment, the patient in his application receives the name of the active substance, for example, "acetylsalicylic acid", "paracetamol" and so on. Knowing him, he can choose the right drug at the nearest DOC + partner pharmacy thanks to the integration of the medication guide. Together with the doctors, we are refining and improving this service.
We also started recording in offline clinics using the application. Now, DOC + clients can sign up for specialists in hospitals.
As for the application for doctors, it is important for us to make the process of filling the cards as easy and fast as possible. One of the upcoming solutions is voice input. Another area of work is the further automation of all routine processes.
We already have about 80 thousand cards. Based on the data stored in them, our machine learning-team teaches the bot to take a history in the process of dialogue with the patient. We are developing some more of our own solutions:
Another area of work is the improvement of the visual part of the medical application. We continue to work to ensure that all users, both patients and doctors, are comfortable working with the system.
In the following materials we will continue to talk about what technologies and developments are behind modern healthcare systems using the example of our DOC + service.
Fortunately, they have a digital alternative - electronic medical records. In this article we will describe how they change the lives of patients and doctors for the better and how we use them to improve the DOC + service.
“ Remember your trips to the clinics. What annoys you about them? ”
What you need to know about electronic medical records?
Electronic medical records, or EHRs, are analogs of paper cards familiar to everyone, which are kept at medical facilities and issued at registries. In the world, they have been running for over 50 years. Their task is to simplify document circulation and reduce the volume of “paper bureaucracy”. The electronic database is easier for doctors to contact, it ensures the completeness of patient data and their safety (in comparison with a paper card that can be lost or messed up, accidentally drops the necessary certificate or a badly pasted sheet).
In the course of treatment or while the patient is using the services of the medical institution, all the same information is entered in the electronic card as in the paper archive - a history of diseases, a history of treatment, data on vaccinations made, and so on. All this information may be available to doctors, clients, and the clinic.
As an EHR product, it is not just a digital version of medical documents, but a full-fledged ecosystem. Doctors, patients and administrative staff work with her. All of them interact with one system, but with different levels of access depending on needs and / or official duties. An EHR for a doctor looks like an analogue of a paper call card with fields for collecting medical information. For the call recipient, as a log entry. For the patient - as his personal medical record.
Why do we need EHR?
For the patient, it is important that the EHRs guarantee the coordinated assistance of all specialists who have ever conducted its examination. Electronic cards provide access to a personal medical history with records in digital form for the entire period of treatment. EHRs reduce the likelihood of medical errors and improve the quality of medical care. The patient gets more control over the treatment process and over their own health - the collected data allow you to track the testimony for the last year or several years. This is useful in emergency cases, and in quite ordinary attempts to lead a healthy lifestyle.
An EHR physician is helped to make the most accurate picture of a patient in the shortest possible time - all data on past diagnoses and prescribed medications are collected in one place. While the doctor is on the way to a call or is waiting for admission in the clinic, he will already know whether the patient has chronic diseases or allergic reactions, which specialists he applied to and what was recommended to him.
For medical institutions EHR is a convenient way to work. Digital records allow you to store information with minimal risk of losing it, reduce the proportion of routine work, solve the problem of overcrowding of archives and help speed up and simplify interaction with other institutions, for example, with insurance companies and other clinics. Researchers at Baylor Scott & White Healthcare Medical Center concluded that the introduction of an EHR at their center helped increase the efficiency of the operating room and reduce the number of delays in preparing for operations.
The digitalization of healthcare (including through the introduction of an EHR) opens up the possibility of automatic data processing and collection of morbidity statistics, which, on the one hand, helps in planning, on the other hand, it increases the level of medical service. Electronic medical records make it easier to control the quality of services through standardization: digitized diagnoses and treatment plans are easier to check for compliance with medical care standards.
It is beneficial for both doctors, patients and clinics that EHRs guarantee the completeness of patient data and their safety. Studies show that large American clinics have reduced their costs by 3.4% three years after adopting the EHR. But in general, American hospitals expect to save up to $ 44 billion a year only due to the introduction of an EHR and a reduction in the number of routine procedures associated with sending, copying and storing paper documents about patients.
If you look wider, e-cards open up the possibility for data exchange between all providers in the health care system. There are already such projects - Taiwan has a system for sharing medical information, Singapore has a national program , and Estonia has a single electronic registry . This, quite likely, awaits us in the future.
Let's sum up the intermediate results. Here are the main advantages of EHR:
- Improving the quality of services provided.
- Data is not lost, it is available and transparent to all interested parties.
- Data is becoming a valuable tool in the treatment and prevention of diseases. Analysts can identify general trends for groups of patients, use statistical data to determine risk factors.
- Medical institutions improve work efficiency - less time is spent on routine and bureaucracy.
- Medicine becomes personalized and more efficient - patients no longer need to tell each doctor their medical history.
And also EHC is eco-friendly. According to the American company Kaiser Permanente, its electronic accounting system has helped to withdraw from circulation 1000 tons of paper documents and 68 tons of X-ray film. For comparison, it is as if 20 thousand Russians in a year would not have spent a single piece of paper.
What medical records does DOC + use?
Our doctors go to home customers, as well as conduct online consultations. For us, EHR is the basis of document flow and a guarantee of a quality service.
DOC + doctors do not take physical cards with them for calls, and the archive is 100% digital. However, by law, we are obliged to keep medical documents in paper form, so the minimum set of required documents is stored in our hub. But the most important thing happens on electronic platforms.
Since the launch of DOC +, the IT system has grown around the project. At first, it was supplemented by a website and applications for doctors and patients. At that time, we made the integration of CRM, call center and medical platform with the backend, and also introduced the prototype of EHR in the usual tables. However, we understood from the very beginning that we would need a complete solution for mobile and desktop devices.
We were guided by the following goals:
- Doctors need a convenient, automated tool in order not to waste time on filling all the fields manually and focus on treatment.
- Patients need to receive examination and test results and have access to their medical history and calls.
- It is important for us to conduct a high-quality medical commission, to evaluate the results of the work of doctors and the correctness of the decisions made.
- We will need all the digitized data in the future to create analytical solutions based on machine learning.
To make this possible, we needed the following basic functionality for doctors:
- Electronic Medical Filling
- Patient records calendar
- Automatically send patient reminders
- The optimal structure of the EHR for doctors of various specializations
- Sending a conclusion to the patient
- View the conclusion in the application
- Billing and payment control
- Electronic directions for analysis
- Direction of prescriptions to convenient pharmacies
- Embedded financial and medical analytics
Patients should immediately have access to:
- His ehm
- Paying bills within the service
- Planning / Transfer / Cancel Calls and Consultations
- Making a call online
The first version of our EHR was focused on the work of pediatricians and therapists. In December 2016, ENTs and neurologists joined DOC +, it became possible to call a nurse and import laboratory test results. The architecture of the solution became more complex, and it became necessary to adapt the maps to the peculiarities of the new specializations. This led us to the creation of the EHC designer. Its development is the next stage of the project.
It took three months to create the first beta version of the EHR system. When she was ready, we moved on to designing a separate mobile application for doctors. Thanks to him, experts can fill the EHR on the service tablets with which they go on calls.
To ensure the safety of user data, all our tablets have a special certified software installed: Continent-AP, Kaspersky Anti-Virus, MDM-center. We made sure that a secure data channel remained between the tablet and our data center.
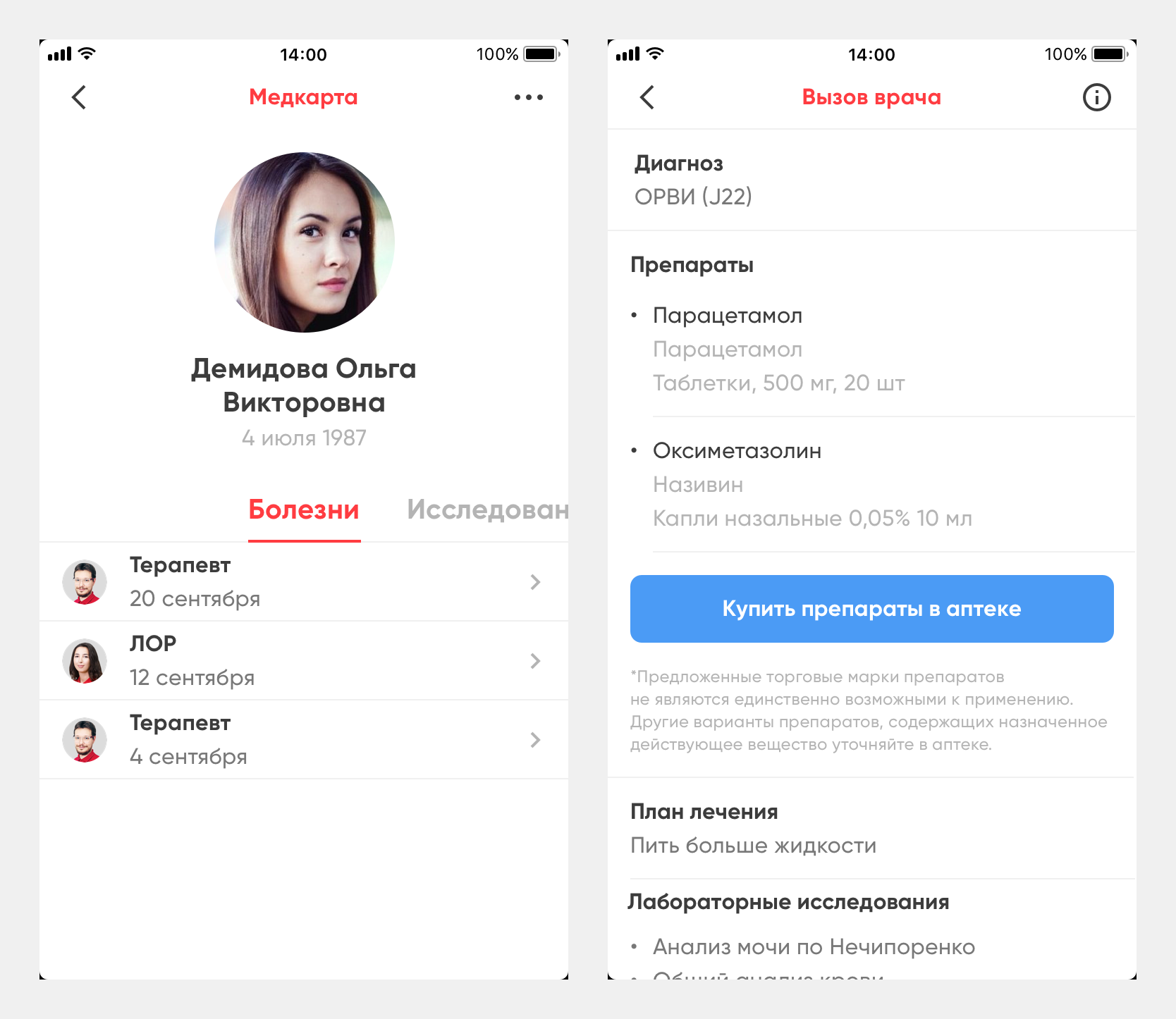
From the client application, the patient learns the diagnosis, the result of the examination by all relevant specialists and the history of calls. In the “Clinic” section, he becomes familiar with the list of our services, and “Chat” allows you to consult with your personal physician.
/ on the screenshot an example of the interface of a personal medical card (as an example, the data of a fictional user is shown)
How do we fill out medical records
The third type of EHR users, besides the doctor and the patient, is the DOC + call center operator. Card management begins with it. Each incoming application from the client - by phone, from the website or from the application - is automatically recorded in CRM. If the application is not received through a mobile application, the call center specialist indicates the name of the applicant and the patient, his address and the doctor’s specialization. If the client has already contacted us before, the name and address are filled in automatically. The operator remains only to clarify them.
As a result, several data blocks are formed at this stage: information about the application, composition of the application, payment information, information about the caller, information about the patient, address of the call with the card, information about the reason for the call, information regarding the disability sheet and the cost of transfer.
All entered data is automatically redirected to the system of auto-dispatching. It is called Mildly Intellectual Routing Algorithm or MIRA. MIRA assigns a specific doctor to the call. The doctor, in turn, receives a formed EHR and assigns the status “on the road” or “drive up”. The customer receives an SMS or push notification that the doctor will arrive soon.
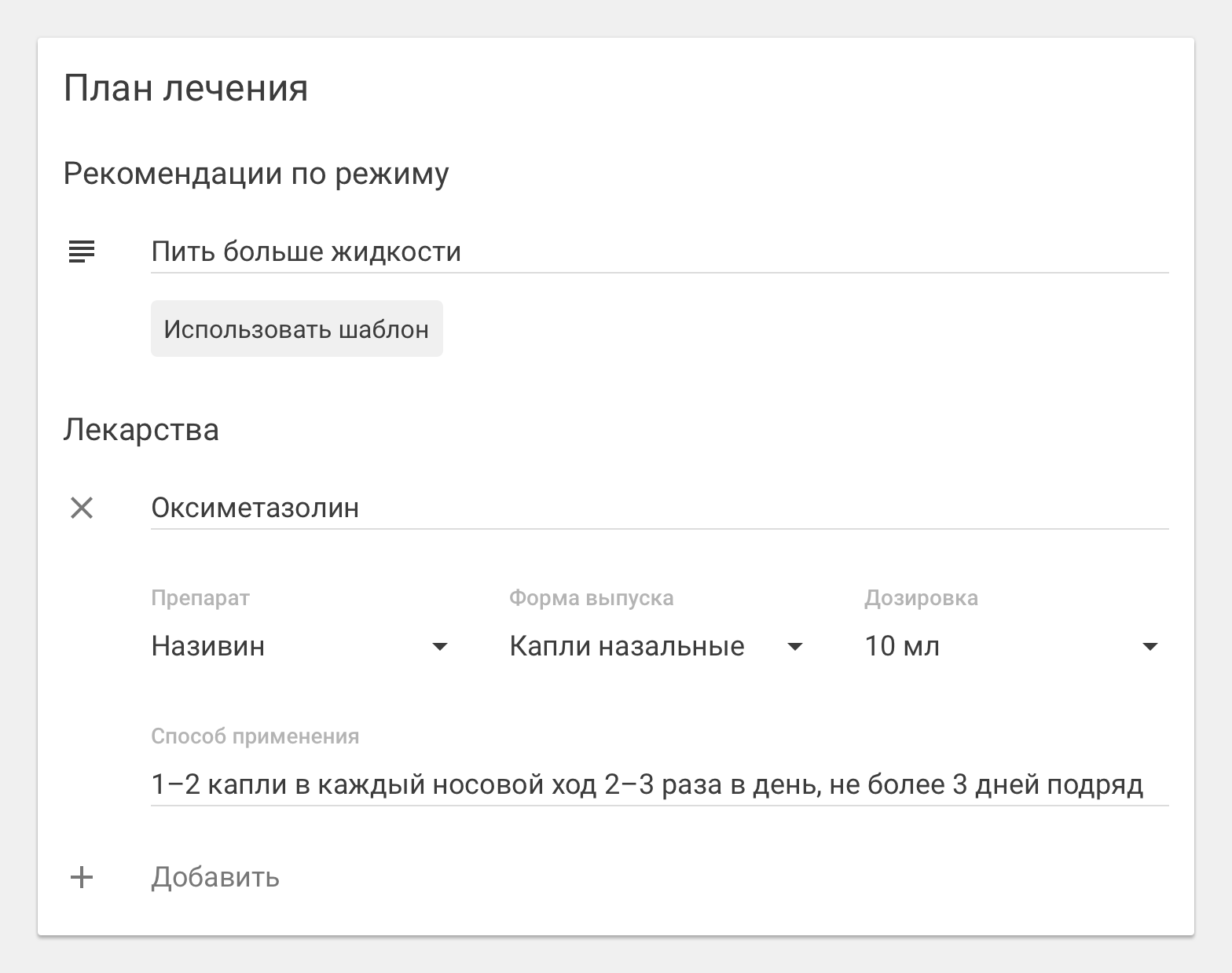
After examining the patient and collecting anamnesis, the doctor fills out the first part of the data in the EHR: client's e-mail, information about referrals to tests or additional studies, diagnosis, and appointments. This information is sent to the client in the DOC + application. In CRM, the diagnosis and prescriptions are not drawn up - this is medical information that the call center operator does not need to know.
/ call window in the DOC + application for doctors (as an example, the data of a fictional user is shown)
In the client application destination appear instantly. The famous problem of "medical handwriting" disappears by itself.
After the call, the doctor fills the card in more detail. Forms of an objective assessment of the general condition of the patient during the inspection of 32 points, the state of the respiratory system on 22 points, the circulatory system on 20 points, as well as the nervous and urogenital systems, blocks of anthropometric data and recommended consultations of relevant specialists are formed. Now for the convenience of making these data provides a drop-down menu with options for answers.
The last stage of the life cycle of an EHR is checking customer well-being Now we are working on the “three calls” system: immediately after the call, in order to clarify how the reception went, in the middle of the recovery process and the final one - by the expected recovery time.
To find out about the client's well-being, call center employees call him on average three days after the inspection. During this time, you can evaluate the first results of treatment. We contact the patient in a convenient way. If he uses only the application, then we will not call him, but write in the chat.
If necessary, the client will be able to talk with the consulting doctor, and the doctor will see if the patient has passed the necessary tests, if he has undergone additional research at a partner clinic.
How EHR helps us to control the quality of medical care
The part of the EHR that is filled in after the call is available to the doctor and the medical board.
The medical commission that controls the quality and safety of medical activities is made up of experts of the relevant specialty who check medical records: whether the medical history is fully collected, whether the prescribed treatment is appropriate for the diagnosis.
Cards are checked for verification by the medical board in an automatic mode, in an impersonal form and randomly. The completed EHR is sent to the common pool, from which the algorithm selects cards for experts.
The commission does not know the identity of the patient, whose card she checks, and the doctor who issued her. Only impersonal information is submitted to the court of experts: medical history, history of the disease, examination data, diagnosis, what treatment the doctor prescribed, what drugs were prescribed, what tests were suggested to be taken, what additional consultations or examinations to take. Verification is conducted by 20 criteria. Each of them is rated on a three-point scale: “fully meets the standards”, “partially meets”, “does not meet”.
The medical commission verifies the correctness of filling the EHR, the completeness of the examination and collection of anamnesis, the compliance of the diagnosis. At the end of the month, the doctor’s accumulative assessment of all his verified cards is considered. We get the assessment of each doctor, groups of doctors, specialties and, in general, all DOC + doctors in the context of different criteria. From the statistics, we learn how correctly doctors choose drugs and treatment. This assessment is used in the scheme of awarding doctors.
How will we develop EHR further?
We have plans to make an EHR more convenient and useful for both the client and the doctor. Now we are focused on expanding the functionality of the cards.
A reference book of drugs has already been added, which contains INN preparations (international non-proprietary name), dosage and release form. After filling the appointment, the patient in his application receives the name of the active substance, for example, "acetylsalicylic acid", "paracetamol" and so on. Knowing him, he can choose the right drug at the nearest DOC + partner pharmacy thanks to the integration of the medication guide. Together with the doctors, we are refining and improving this service.
We also started recording in offline clinics using the application. Now, DOC + clients can sign up for specialists in hospitals.
As for the application for doctors, it is important for us to make the process of filling the cards as easy and fast as possible. One of the upcoming solutions is voice input. Another area of work is the further automation of all routine processes.
We already have about 80 thousand cards. Based on the data stored in them, our machine learning-team teaches the bot to take a history in the process of dialogue with the patient. We are developing some more of our own solutions:
- automatic quality control system. It will increase the productivity of the medical commission and will allow you to check not 15-20%, but 100% of all EHRs;
- decision support system for doctors. It will reduce the likelihood of errors and effectively lead all services to a single standard. In addition, this solution will help control appointments for compliance with evidence-based medicine.
Another area of work is the improvement of the visual part of the medical application. We continue to work to ensure that all users, both patients and doctors, are comfortable working with the system.
In the following materials we will continue to talk about what technologies and developments are behind modern healthcare systems using the example of our DOC + service.
All Articles